Impact of clinical signs and genetic diagnosis of familial hypercholesterolaemia on the prevalence of coronary artery disease in patients with severe hypercholesterolaemia
 Tada H, Kawashiri MA, Nohara A, Inazu A, Mabuchi H, Yamagishi M.
Tada H, Kawashiri MA, Nohara A, Inazu A, Mabuchi H, Yamagishi M.
Eur Heart J. 2017 May 21;38(20):1573-1579. ![]()
Impact Factor (2016): 19.651![]()
日常診療において多く遭遇する高コレステロール血症を呈する患者群から、家族性高コレステロール血症を正しく診断することは、冠動脈疾患の予防管理において重要なことであると臨床的には実感されてきました。
本論文ではこの臨床的な感覚を多数例の高コレステロール血症患者の臨床像、遺伝的背景を解析することで科学的に証明した意義深い論文です。
多田助教は本論文にて第81回 日本循環器学会学術集会YIA(臨床部門)最優秀賞を受賞する快挙を成し遂げています。
多田助教はHarvard大学(Masatuesettu General Hospital)留学中の仕事でもEuropean Heart Journalに論文が採択されています。
>【原著論文】冠動脈疾患のリスク予測においてGenetic Risk Scoreは家族歴を凌駕する

Aims
The impact of positive clinical signs (xanthoma and/or family history) and positive familial hypercholesterolaemia (FH) mutation status on risk of coronary artery disease (CAD) over and above that predicted by low-density lipoprotein (LDL) cholesterol level alone has not been fully determined. We assessed whether positive clinical signs and genetic FH diagnosis affected CAD risk among subjects with significantly elevated LDL cholesterol levels (≥180 mg/dL, or ≥140 mg/dL in subjects <15 years of age).
Three genes causative for FH (LDLR, APOB, and PCSK9) were sequenced in 636 patients with severe hypercholesterolaemia (mean age, 45 years; 300 males [47%], CAD diagnosis, 185 [29%]), and the presence of clinical FH signs (xanthoma and/or family history) were assessed. CAD prevalence was compared between four subject groups categorized based on these parameters.
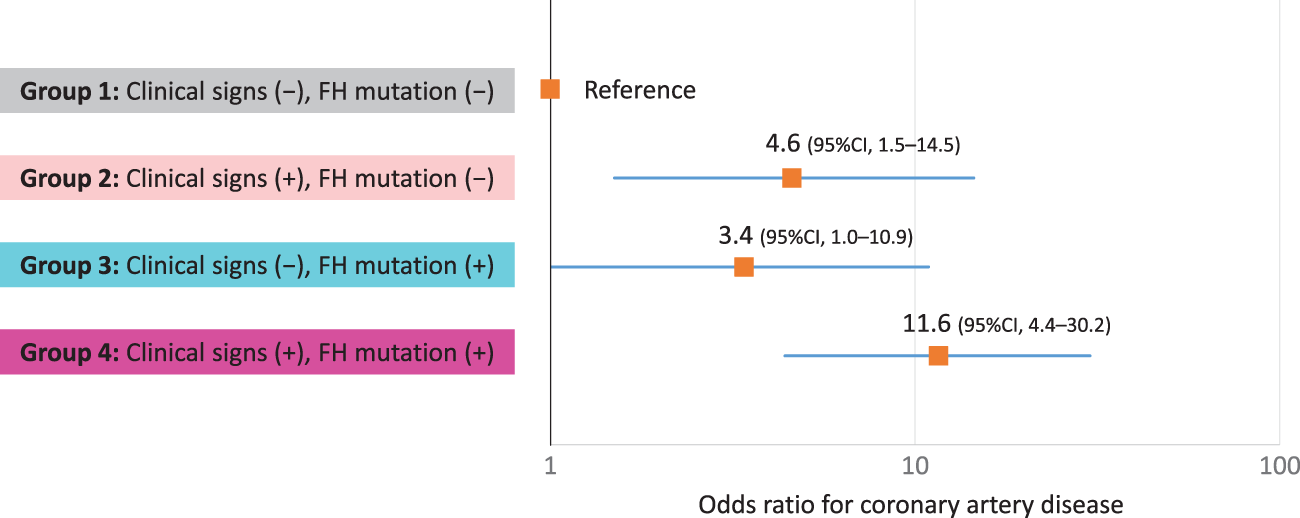
Compared with the reference group without FH mutations or clinical signs of FH, subjects with clinical signs of FH or FH mutations had three- to four-fold higher odds of developing CAD (odds ratio [OR], 4.6; 95% confidence interval [CI], 1.5–14.5; P = 0.0011 and OR, 3.4; 95% CI, 1.0–10.9; P = 0.0047, respectively), whereas those with clinical signs of FH and FH mutation(s) had >11-fold higher odds of developing CAD (OR, 11.6; 95% CI, 4.4–30.2; P = 1.1 × 10−5) after adjusting for known risk factors including LDL cholesterol.
Our findings revealed an additive effect of positive clinical signs of FH and positive FH mutation status to CAD risk among patients with significantly elevated LDL cholesterol.