金沢大学臓器機能制御学教室では、教育、臨床とともに基礎、臨床研究にも力を注いでいます。昨年末から今年にかけまして、国際共同研究、金沢大学内臨床研究、さらにパンチの効いた症例報告論文が相次いで発表されました。中でも直近のEur Heart Jは現在IF>14の難関誌で、筆頭著者のHideki Itoh (伊藤英樹)氏も元をたどれば、金沢大学出身です。また、当科の林 研至助教などが共同研究者となっています。
Itoh H, Crotti L, Aiba T, Spazzolini C, Denjoy I, Fressart V, Hayashi K, Nakajima T, Ohno S, Makiyama T, Wu J, Hasegawa K, Mastantuono E, Dagradi F, Pedrazzini M, Yamagishi M, Berthet M13, Murakami Y, Shimizu W15, Guicheney P, Schwartz PJ, Horie M
The genetics underlying acquired long QT syndrome: impact for genetic screening.
Eur Heart J. 2015 Dec 28. pii: ehv695. [Epub ahead of print]
http://eurheartj.oxfordjournals.org/content/early/2015/12/28/eurheartj.ehv695.long
Abstract
AIMS: Acquired long QT syndrome (aLQTS) exhibits QT prolongation and Torsades de Pointes ventricular tachycardia triggered by drugs, hypokalaemia, or bradycardia. Sometimes, QTc remains prolonged despite elimination of triggers, suggesting the presence of an underlying genetic substrate. In aLQTS subjects, we assessed the prevalence of mutations in major LQTS genes and their probability of being carriers of a disease-causing genetic variant based on clinical factors.
METHODS AND RESULTS: We screened for the five major LQTS genes among 188 aLQTS probands (55 ± 20 years, 140 females) from Japan, France, and Italy. Based on control QTc (without triggers), subjects were designated ‘true aLQTS’ (QTc within normal limits) or ‘unmasked cLQTS’ (all others) and compared for QTc and genetics with 2379 members of 1010 genotyped congenital long QT syndrome (cLQTS) families. Cardiac symptoms were present in 86% of aLQTS subjects. Control QTc of aLQTS was 453 ± 39 ms, shorter than in cLQTS (478 ± 46 ms, P < 0.001) and longer than in non-carriers (406 ± 26 ms, P < 0.001). In 53 (28%) aLQTS subjects, 47 disease-causing mutations were identified. Compared with cLQTS, in ‘true aLQTS’, KCNQ1 mutations were much less frequent than KCNH2 (20% [95% CI 7-41%] vs. 64% [95% CI 43-82%], P < 0.01). A clinical score based on control QTc, age, and symptoms allowed identification of patients more likely to carry LQTS mutations.
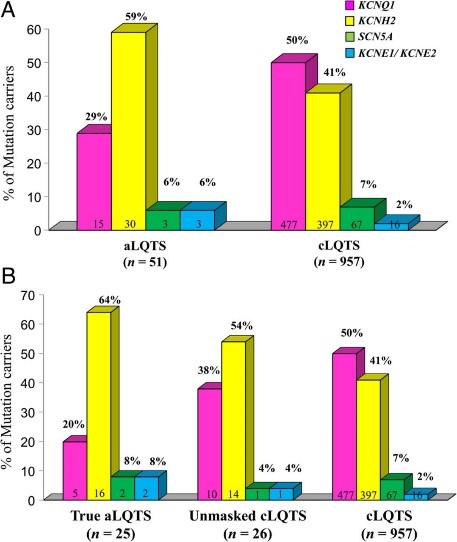 CONCLUSION: A third of aLQTS patients carry cLQTS mutations, those on KCNH2 being more common. The probability of being a carrier of cLQTS disease-causing mutations can be predicted by simple clinical parameters, thus allowing possibly cost-effective genetic testing leading to cascade screening for identification of additional at-risk family members.
CONCLUSION: A third of aLQTS patients carry cLQTS mutations, those on KCNH2 being more common. The probability of being a carrier of cLQTS disease-causing mutations can be predicted by simple clinical parameters, thus allowing possibly cost-effective genetic testing leading to cascade screening for identification of additional at-risk family members.
Konno T, Nagata Y, Teramoto R, Fujino N, Nomura A, Tada H, Sakata K, Furusho H, Takamura M, Nakamura H, Kawashiri MA2 Yamagishi M, Hayashi K.
Usefulness of Electrocardiographic Voltage to Determine Myocardial Fibrosis in Hypertrophic Cardiomyopathy.
Am J Cardiol. 2015 Nov 19. pii: S0002-9149(15)02253-5. doi: 10.1016/j.amjcard.2015.11.015. [Epub ahead of print]
http://www.sciencedirect.com/science/article/pii/S0002914915022535
 Abstract
Abstract
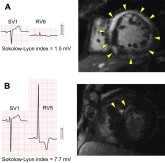
Classic electrocardiographic (ECG) voltage indexes have been applied to screen for left ventricular (LV) hypertrophy in hypertrophic cardiomyopathy (HC). However, it is unclear whether low ECG voltage reflects deteriorated electrical forces because of replacement of the myocardium by fibrotic tissues in HC. We investigated correlations between classic ECG voltage indexes (Cornell, total QRS voltage, and Sokolow-Lyon) and cardiac magnetic resonance (CMR) parameters focusing on the impact of low ECG voltage on the LV ejection fraction (LVEF) and myocardial fibrosis in HC. We studied 108 consecutive patients with HC who underwent CMR imaging with late gadolinium enhancement (LGE). Nineteen patients with complete right or left bundle branch block were excluded, leaving 89 patients for analysis (age 61.0 ± 13.9 years; 58 men). Of the 3 voltage indexes, the total QRS voltage and Sokolow-Lyon indexes were positively correlated with LVEF. For discriminating patients with end-stage HC (LVEF <50%) from patients with HC and preserved LVEF (≥50%), receiver-operating characteristic analysis revealed an excellent area under the curve of 0.87 for the total QRS voltage index and 0.90 for the Sokolow-Lyon index, whereas the area under the curve for the Cornell index was only 0.54 (p <0.01). Moreover, these 2 voltage indexes were negatively correlated with the extent of LGE-determined myocardial fibrosis when adjusted by the LV maximal wall thickness. In conclusion, low ECG voltage indexes may reflect increased myocardial fibrosis in patients with HC.
Nakahashi T1, Sakata K1, Tsuda T1, Tanaka Y1, Ohira M1, Mori M1, Takata M1, Kawashiri MA1, Takemura H1, Yamagishi M1, Hayashi K1.
Abrupt progression of ventricular septal perforation after primary angioplasty for acute myocardial infarction.
Cardiovasc Diagn Ther. 2015 Dec;5(6):479-83. doi: 10.3978/j.issn.2223-3652.2015.06.06.
http://www.ncbi.nlm.nih.gov/pubmed/26675980
Abstract
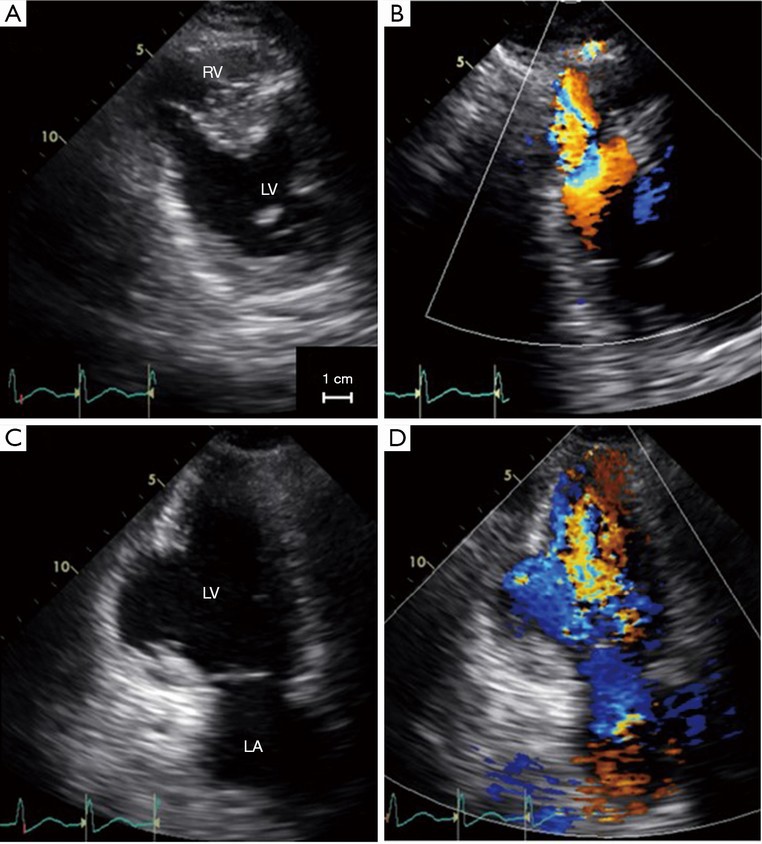 A 61-year-old-man was transferred to our hospital because of progressive heart failure after reperfusion for acute myocardial infarction (MI). When he visited the local hospital with severe chest pain associated with inferior MI, transthoracic echocardiography revealed small ventricular septal perforation (VSP). The patient had emergent coronary angiography, which revealed total occlusion of the mid-portion of the right coronary artery. Primary angioplasty was successful for reperfusion. However, because of hemodynamic instability the patient was transferred to our hospital. Under these conditions, transthoracic echocardiography which was undertaken 3 hours after primary angioplasty, demonstrated progressive enlargement of the VSP probably due to reperfusion injury. The rupture site, which was further enlarged at the time of operation, was repaired using the patch exclusion technique. The patient could discharge without complications. We suggest that primary angioplasty may potentially induce late reperfusion injury in patients with VSP complicating MI.
A 61-year-old-man was transferred to our hospital because of progressive heart failure after reperfusion for acute myocardial infarction (MI). When he visited the local hospital with severe chest pain associated with inferior MI, transthoracic echocardiography revealed small ventricular septal perforation (VSP). The patient had emergent coronary angiography, which revealed total occlusion of the mid-portion of the right coronary artery. Primary angioplasty was successful for reperfusion. However, because of hemodynamic instability the patient was transferred to our hospital. Under these conditions, transthoracic echocardiography which was undertaken 3 hours after primary angioplasty, demonstrated progressive enlargement of the VSP probably due to reperfusion injury. The rupture site, which was further enlarged at the time of operation, was repaired using the patch exclusion technique. The patient could discharge without complications. We suggest that primary angioplasty may potentially induce late reperfusion injury in patients with VSP complicating MI.